
Reconstitution Requires Reckoning: The Brains We Are Rewriting
“We have documented the neurological damage. Now we must impose consequences on the incentives that profit from it. Reckoning without enforcement is just another form of delay.”


Last week we described how the machinery operates. We showed the 1960s compact that lacks any real enforcement power, the routine failure to meet the 60-day home study deadline, the Title IV-E funding structure that reimburses states and providers at dramatically higher rates for congregate and residential placements than for kinship care, and the documented cases in Indiana where caseworkers admitted under oath to deliberately avoiding ICPC filings because they viewed the process as creating unwanted “roadblocks.” We saw children like the two boys still separated from their grandmother and aunt in Indiana while the paperwork moved at its own pace. That article explained the architecture of delay. This one examines what that architecture is actually doing to the children trapped inside it.
The evidence compiled in Section 6 of the Project Milk Carton investigation is not theoretical. It is drawn from systematic reviews, neuroscience research, and longitudinal outcome data. It shows that prolonged ICPC delays and the institutional placements they produce create measurable biological changes in children’s brains, fracture attachment systems at rates far above the general population, expose children to significantly elevated risks of sexual abuse in group settings, drive heavy psychotropic medication use that often manages symptoms rather than addressing root causes, and contribute directly to the catastrophic life outcomes experienced by thousands of youth who age out of foster care without permanency each year. These are not unfortunate side effects of an otherwise functional system. They are predictable, dose-dependent consequences of a process that keeps children in the most expensive and most harmful placements while relatives wait.
Placement Instability as a Predictable Driver of Harm
A 2024 systematic review published in the Journal of Child & Adolescent Trauma synthesized fourteen peer-reviewed studies and reached a clear conclusion: placement instability is one of the most consistent predictors of poor outcomes across multiple domains for children in foster care. Children who experienced five or more placement changes showed significantly greater internalizing and externalizing behavioral difficulties compared to those with fewer moves. Males with three or more placements were 1.54 times more likely to have delinquency petitions filed against them. Placement instability also predicted higher likelihood of screening positive for PTSD, depression, and substance use disorders.
The relationship is bidirectional and self-reinforcing. Instability creates behavioral problems. Those behavioral problems increase the chance of another placement disruption. Each new disruption adds another layer of loss and stress. Children who achieved stable placement within forty-five days showed between 36 and 63 percent better behavioral scores at eighteen months, depending on their starting severity. When ICPC processing times stretch to six months or longer, as they routinely do in many states, children lose that protective window. The research makes clear that the longer the delay, the greater the accumulated damage.
This is not simply a matter of children being “upset” by moving. The instability itself becomes a source of trauma that compounds the original removal. Every new placement requires the child to adapt to new caregivers, new rules, new environments, and often new schools. For children whose early development has already been disrupted by removal from their birth parents, these repeated ruptures make it increasingly difficult to form trusting relationships or develop a coherent sense of safety. The system that claims to protect children is, through its own processes, actively multiplying the number of relational losses they must absorb.
The Neurobiological Record of Harm
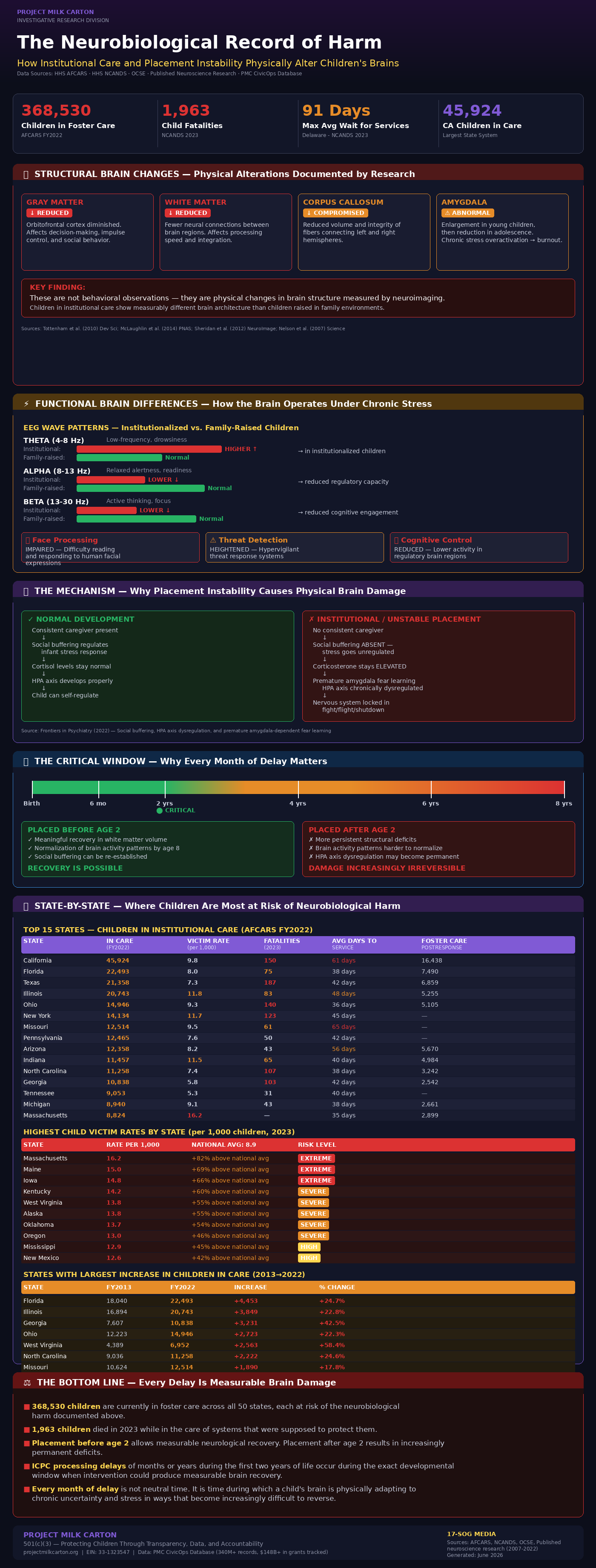
The damage is not limited to observable behavior. Neuroscience research documents physical changes in brain structure and function among children who experience institutional care and high levels of placement instability. Studies have found reduced volumes of both gray and white matter in children raised in institutional settings compared to those raised in family environments. The corpus callosum, the major bundle of fibers connecting the brain’s two hemispheres, shows reduced volume and integrity. Gray matter in the orbitofrontal cortex, a region heavily involved in decision-making, impulse control, and the regulation of social behavior, is diminished. Amygdala development follows a troubling pattern: enlargement in younger children followed by reduction in adolescence, consistent with chronic stress-driven overactivation followed by burnout.
Functional differences are equally concerning. Institutionalized children show atypical patterns of brain activity, including higher power in low-frequency theta bands and lower power in the mid-to-high frequency alpha and beta ranges. Their brains are, in measurable electrophysiological terms, operating at a lower level of efficiency in key regulatory bands. Face processing is impaired, meaning children have greater difficulty accurately reading and responding to human facial expressions. Threat detection systems are heightened, while activity in regions responsible for cognitive control is reduced. These patterns are not minor variations. They represent measurable alterations in how the brain processes social information and manages stress.
A 2022 paper in Frontiers in Psychiatry provides insight into the mechanism. In typical development, the presence of a consistent caregiver helps regulate the infant’s stress response through a process called social buffering. When this buffering is absent or unreliable, as it is during extended periods of institutional care or repeated placement changes, stress hormones remain elevated even in the presence of adults. Elevated corticosterone can prematurely activate amygdala-dependent fear learning before the brain is developmentally prepared for it. Over time, this contributes to a chronically dysregulated HPA axis, the body’s central stress response system. The result is a nervous system that is more easily triggered into states of fear or shutdown and less capable of returning to calm.
The timing of these experiences matters enormously. Research indicates that children placed into stable, high-quality family care before the age of two show meaningful recovery in white matter volume and normalization of certain brain activity patterns by age eight. Children placed after this early window show more persistent deficits. ICPC delays that extend for months or years during the first two years of life are therefore occurring during the precise developmental period when intervention could still produce measurable neurological recovery. Every month of delay during this window is not neutral time. It is time during which the child’s brain is adapting to conditions of chronic uncertainty and stress in ways that can become increasingly difficult to reverse
.
Attachment Disruption as a Core Wound
Every placement change represents the loss of another attachment figure. For children who have already been removed from their birth parents, these subsequent losses compound the original trauma rather than allowing healing to begin. The research literature documents this as one of the most damaging aspects of foster care instability.
Reactive Attachment Disorder appears at approximately five percent prevalence among children upon entry into foster care, a rate two and a half to five times higher than in the general population. Disinhibited Social Engagement Disorder, characterized by indiscriminate friendliness, lack of appropriate boundaries with strangers, and difficulty forming selective attachments, appears in 30.9 percent of foster children. These are not random behavioral issues. They reflect the child’s adaptation to environments in which consistent, safe, and responsive caregiving could not be relied upon. Children with multiple placement changes show the highest rates of these attachment disturbances.
Importantly, the research also shows that stability can produce recovery. Following at least one year of stable, improved care, the prevalence of Reactive Attachment Disorder drops significantly. This demonstrates that the harm is not inevitable and that stability itself functions as a powerful intervention. The tragedy of the current ICPC system is that it systematically delays or prevents the very placement type that research identifies as most protective for children’s attachment development.
The implications extend far beyond childhood. Disrupted attachment in early years affects the capacity to form healthy relationships, regulate emotions, and trust others throughout life. When a system keeps children in conditions of repeated relational rupture while relatives who are willing and vetted wait months or years for approval, it is not merely slowing down a bureaucratic process. It is actively interfering with the conditions children need to develop the internal architecture required for healthy human connection.
Mental Health Outcomes and the Dose-Dependent Pattern
The mental health data reveals clear, elevated risks. Foster children experience PTSD at rates around 30 percent compared to 7.6 percent in the general population. Depression diagnoses appear at roughly 41 percent versus 18 percent among youth generally. ADHD diagnoses occur at approximately three times the base rate. Developmental delays appear at roughly twice the general population rate. Children with five or more placements show psychiatric disorder rates more than six times higher than children who experience only a single stable placement.
These are not small differences. They represent a dramatically higher burden of suffering and impairment. Youth with foster care experience are up to 62 percent more likely to face significant mental health challenges, including depression, anxiety, and PTSD, than their peers. The suicide risk among foster youth ranks among the highest of any identifiable population in the country.
The pattern is dose-dependent. More placement instability and more time in institutional settings correlate with worse outcomes across nearly every measured domain. This is not surprising once the neurobiological and attachment research is taken seriously. When a child’s developing stress response system is repeatedly activated without adequate regulation, when attachment figures are lost multiple times, and when the environment provides little predictability or safety, the child’s internal resources for managing distress become depleted. Behavioral and emotional symptoms are the predictable result.
The Heightened Risks of Congregate Care
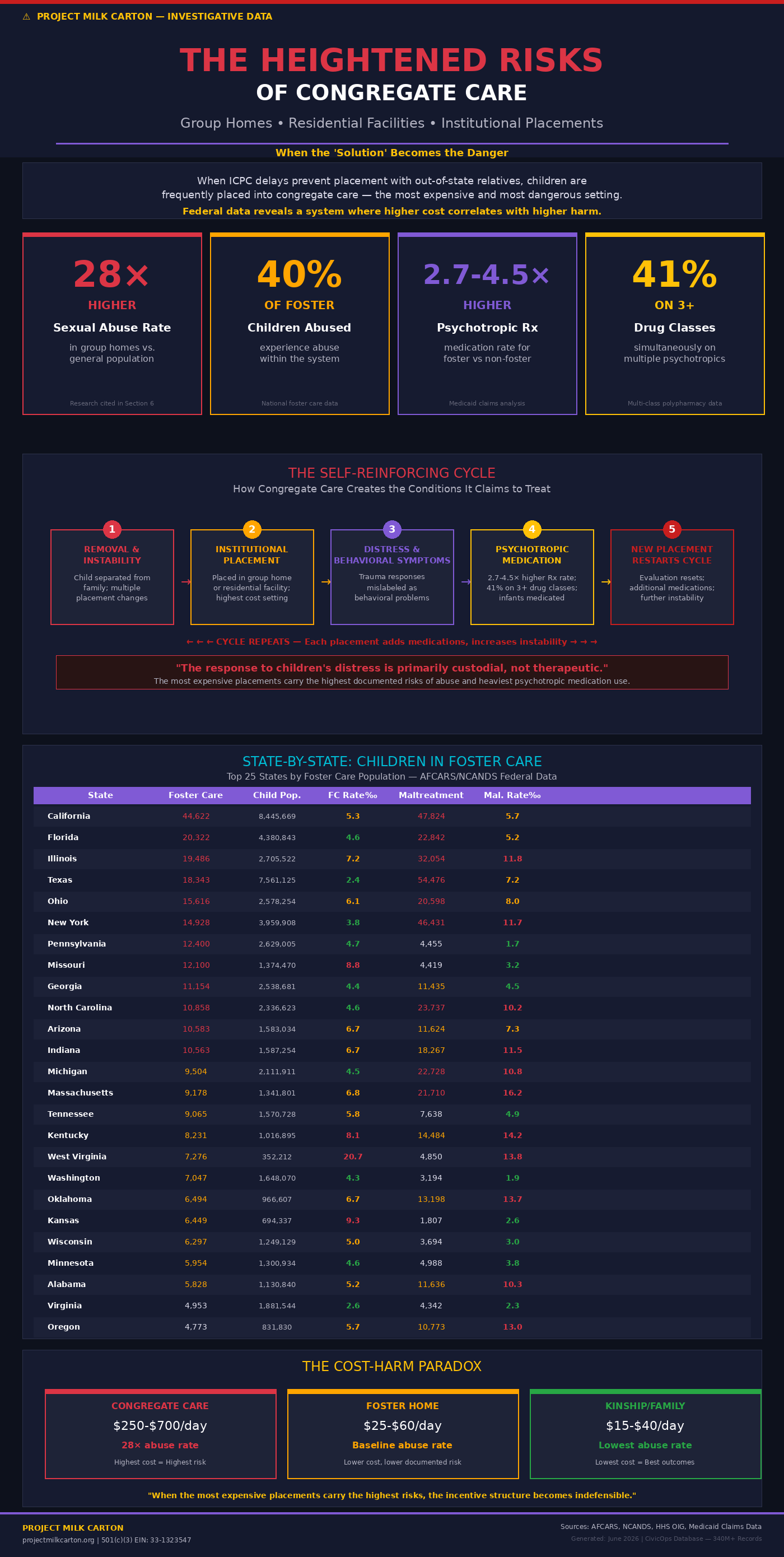
When ICPC delays prevent placement with out-of-state relatives, children are frequently kept in or moved into congregate care settings such as group homes and residential treatment facilities. These environments carry risks that extend well beyond their high cost. Research cited in the Section 6 analysis shows that sexual abuse rates in group homes are 28 times higher than in the general population. Up to 40 percent of children in foster care experience some type of abuse within the system itself. Twenty percent of substantiated sexual abuse cases in foster care involve foster parents or caregivers as perpetrators. Girls in particular experience abuse with greater frequency and repetition.
The behavioral symptoms that often emerge in these settings are frequently addressed through psychotropic medication. Foster children in Medicaid are prescribed these drugs at rates 2.7 to 4.5 times higher than non-foster children. Forty-one percent of medicated foster children are simultaneously on three or more different classes of psychotropic medications. Even infants under one year of age in foster care receive these prescriptions at elevated rates. The cycle is self-reinforcing: removal and instability create distress, institutional placement often intensifies that distress, medication is used to manage the resulting behavior, and each new placement may restart the evaluation process, sometimes adding additional medications.
This pattern raises serious questions about whether the response to children’s distress is primarily therapeutic or primarily custodial. When the most expensive placements also carry the highest documented risks of abuse and the heaviest use of psychotropic medication, the incentive structure that directs children into those placements becomes even more difficult to defend.
Aging Out and the Lifetime Costs of Systemic Failure
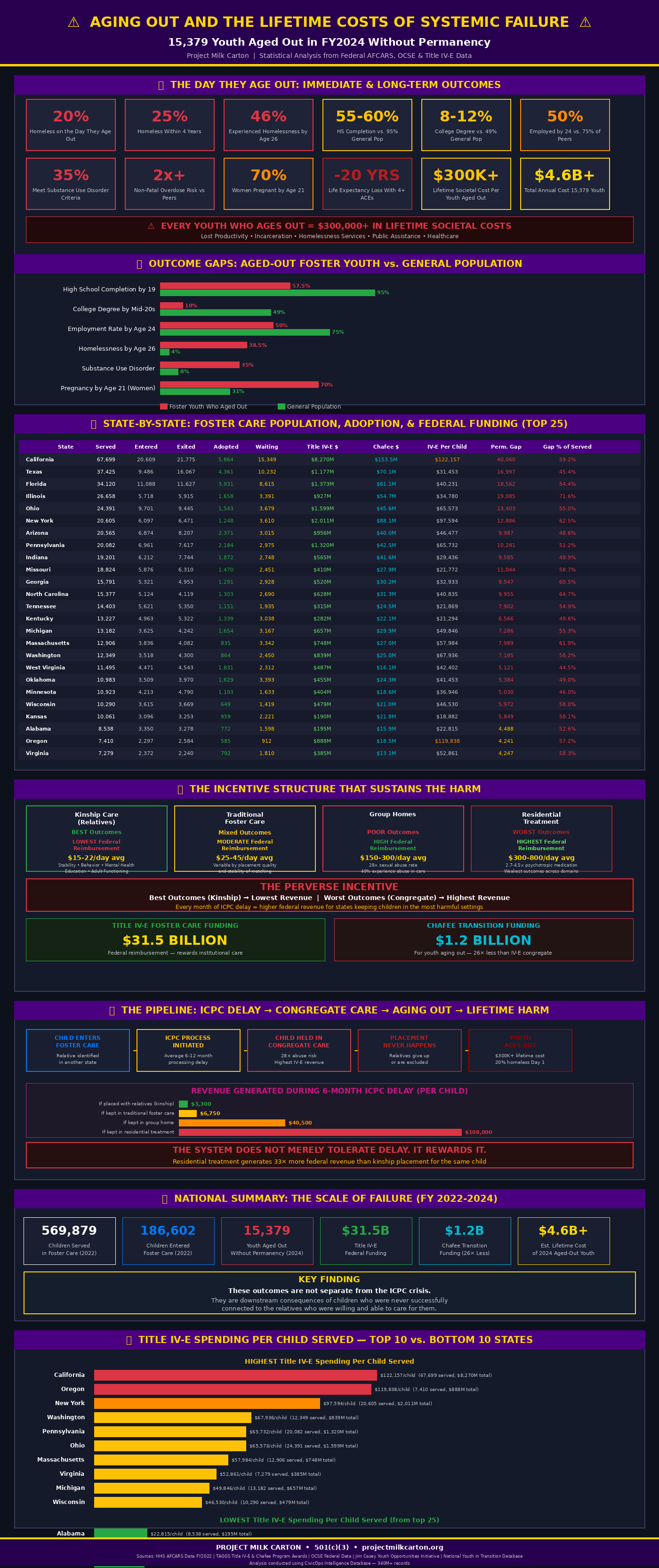
In fiscal year 2024, 15,379 youth aged out of foster care without ever achieving permanency. These are children the system failed to connect with families, often because interstate barriers and related processes prevented timely kinship placement during the years when it could have made the greatest difference. The outcomes for this group are severe and well-documented.
Twenty percent become homeless on the day they age out. Twenty-five percent experience homelessness within four years. By age 26, between 31 and 46 percent have experienced homelessness. High school completion by age 19 stands at 55 to 60 percent, compared to 95 percent in the general population. College degree attainment by the mid-to-late twenties is only 8 to 12 percent, versus 49 percent generally. By age 24, only about half are employed, compared to 75 percent of their peers, and their earnings are roughly half as high. Substance use disorder criteria are met by 35 percent, with non-fatal overdose risk more than twice as high as peers. Seven out of ten women who aged out become pregnant by age 21.
People who experience four or more Adverse Childhood Experiences lose approximately twenty years of life expectancy on average compared to those with fewer. Children in foster care typically accumulate multiple ACEs before entering care and then add more through placement disruptions, institutional environments, and the medication patterns described above. Every youth who ages out without permanency represents an estimated lifetime societal cost exceeding $300,000 in lost productivity, incarceration, homelessness services, and public assistance.
These outcomes are not separate from the ICPC crisis. They are downstream consequences of children who were never successfully connected to the relatives who were willing and able to care for them.
The Incentive Structure That Sustains the Harm
The financial architecture of the current system reinforces rather than mitigates these outcomes. Kinship care with relatives produces the best documented results across stability, behavioral outcomes, mental health, educational attainment, and adult functioning, yet it generates the lowest level of federal reimbursement. Residential treatment and congregate care produce the weakest outcomes across nearly every domain, yet they generate the highest levels of federal reimbursement through Title IV-E. States and providers receive more federal dollars the longer children remain in the most expensive and most harmful settings.
This is not a neutral funding mechanism. It is a structure that creates direct financial incentives to maintain children in placements that research shows are most damaging. When ICPC delays keep children in congregate care for additional months, those months generate substantially higher federal revenue for the state and the placement provider than the same months would generate if the child were placed with relatives. The system does not merely tolerate delay. In measurable financial terms, it rewards it
.
Why This Evidence Demands Reckoning
Last week’s article showed how the machinery of removal and delay functions with minimal accountability. This evidence shows what that machinery produces inside children’s developing brains and across their life trajectories. A reconstitution effort that does not directly confront these outcomes cannot claim seriousness about protecting children or families. Constitutional accountability requires that when the state exercises the extraordinary power to separate children from their kin, it does so under conditions that minimize rather than maximize documented harm. Enforceable timelines, genuine preference for kinship placement, transparent measurement of developmental impact, and financial consequences for chronic violation of legal standards are not optional enhancements. They are baseline requirements for any system that claims to act in children’s best interests.
The current absence of systematic tracking of what happens to children’s neurological development, attachment security, and long-term functioning under different placement timelines is not a minor administrative gap. It is a form of institutional self-protection that allows documented harm to continue without consequence or correction.
What Reckoning Requires
States must be required to publicly report ICPC processing times, denial rates disaggregated by relationship type, and longitudinal outcomes for children subject to interstate delays. Federal enforcement mechanisms with meaningful financial consequences for chronic violation of the 60-day home study deadline must be established. Provisional kinship placement authority, allowing vetted relatives to receive children within days rather than months pending full approval, should replace prolonged institutional holding patterns. Kinship stipend parity must eliminate the financial penalty families currently face for stepping forward to care for their relatives’ children. Any predictive risk tools or assessment instruments used to justify removal or to evaluate relatives must be subject to independent validation, public scrutiny, and ongoing outcome measurement.
Most fundamentally, the system must be required to measure and disclose what actually happens to children’s development when delays occur and when children are placed in different settings. Without that measurement, claims that current practices serve children’s best interests remain untestable and therefore unaccountable.
The Standard We Must Apply
The children caught in ICPC delays are not administrative units or funding units. Their brains are developing under conditions that research shows can produce lasting alterations in stress regulation, emotional control, and the capacity for relationship. The attachment disruptions, elevated exposure to abuse in congregate settings, and patterns of heavy psychotropic medication are measurable realities. The lifetime costs to those children and to the society they will join are documented and substantial.
Reconstitution that treats this evidence as secondary or as an unfortunate but unavoidable cost of doing business cannot succeed. The data shows that current practices are not neutral. They are actively producing harm in predictable, dose-dependent ways while directing the highest levels of public funding toward the placements with the weakest results. A republic that claims to value the family as its foundational unit cannot continue to accept measurable damage to children’s developing minds as the routine output of its child welfare processes.
The research has been done. The patterns are clear. The harm is not theoretical. It is occurring on our watch, with our funding, under legal frameworks that were written to protect children but are currently operating without meaningful accountability for the damage they produce. Reconstitution begins when we stop pretending otherwise and insist that protecting children requires protecting their brains, their attachments, and their futures from processes that demonstrably harm them.
The evidence leaves no comfortable middle ground. Either we reckon with what the research shows and rebuild accordingly, or we continue to manage a system that rewrites children’s brains while claiming to protect them. The choice is not between compassion and fiscal responsibility. It is between continuing to produce documented harm and finally aligning our practices, our incentives, and our accountability structures with what children actually need.
If you enjoyed this work and feel encouraged by independent investigations like this, please consider becoming a paid subscriber to The Constitutional Republic on Substack or donate at
Project Milk Carton Inc. Your gift keeps our site alive, spotlighting high-risk children!
Your support helps us continue:
investigative reporting
public records research
educational transparency projects
community outreach
and future investigations like this series
Most importantly, please share this article.
Independent journalism survives when ordinary people help spread information powerful institutions would prefer to remain ignored, misunderstood, or buried beneath complexity.
Because silence protects systems.
Informed communities protect children.
ALL paid subscriptions are tax deductible Project Milk Carton | 501(c)(3) | EIN: 33-1323547
This Substack is reader-supported. To receive new posts and support my work, consider becoming a free or paid subscriber.
SOURCES & CITATIONS
[1] Systematic Review: Placement Instability & Behavioral/Emotional Outcomes Journal of Child & Adolescent Trauma, 2024. PMC 11199447. 14 studies reviewed.
[2] Neurobiology of Infant Attachment-Trauma Frontiers in Psychiatry, 2022. PMC 9352889. Sullivan et al.
[3] Out-of-Home Care and Brain Development Child and Adolescent Psychiatry and Mental Health, 2024. PMC 10995925.
[4] Reactive Attachment Disorder in Foster Children Attachment & Human Development, 2019. PubMed 30021488.
[5] Attachment Disorder Symptoms and Associations Child and Adolescent Psychiatry and Mental Health, 2023. PMC 10422696.
[6] Foster Care, Permanency, and Risk of Prison Entry Children and Youth Services Review, 2022. PMC 8975219. Wisconsin study, N=10,000+.
[7] Sexual Abuse of Children in U.S. Foster Care Ballard Brief, BYU. Johns Hopkins University study cited.
[8] GAO: Psychotropic Medication in Foster Care GAO-12-201 (2012), GAO-14-651t (2014), GAO-17-129 (2017).
[9] Aging Out Outcomes Blue Ribbon Project, 2024. Annie E. Casey Foundation. NYTD data.
[10] Foster Care & Child Maltreatment Mortality JAMA Network Open, 2025. PMC 12754682. 3.4M records, 2010-2023.
[11] Kinship Care Stability & Outcomes Chapin Hall Policy Brief, 2023. Casey Family Programs.
[12] Cost of Foster Care Father's Advocacy Network, 2024. HHS/Title IV-E rate data.
[13] Foster Care Abuse Statistics Penny Lane Centers, 2024. Focus for Health, 2024.
[14] ACEs and Brain Development PMC 8882933 (2022). Cleveland Clinic. Aetna Better Health.
[15] ICPC Delay Data Foster Focus Magazine. ABA Child Law Practice, 2014. National Council of Juvenile and Family Court Judges.
[16] PMC CivicOps Database IRS Form 990 Schedule I (630,263 grants, $89.1B); TAGGS NGO Grants (22,960 grants, $58.6B); USASpending Subawards (1,046,123 records, $1B+)
The preamble is even edited when I go to the National Archives.